

Hearing is an essential sensory skill for the acquisition of communication ability in a child. Overlooked hearing problems in newborn babies and children will lead to delayed interventions resulting in poor language and cognitive (intelligence) outcomes. In this article, I want to inform parents about hearing problems in children with an emphasis on hearing screening tests in newborns and infants.
How common are hearing problems in newborns and children?
The reported rate of hearing problems in newborn babies is 1-2 cases per 1000 births. However, by school age, we will have diagnosed 5-6 children with hearing deficits.
The incidence of hearing problems at birth is lower than at school age because current screening methods may miss some cases of milder hearing deficits. Furthermore, some babies acquire hearing deficits later after birth, or they have progressive hearing loss that gets worse over time.
How do we hear sounds?
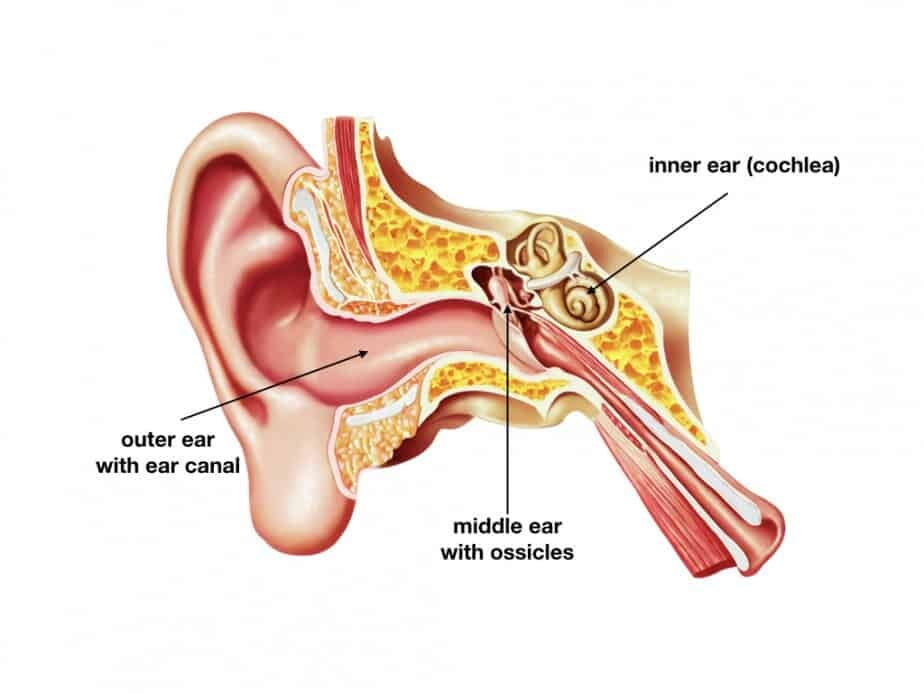
In the process of hearing, we utilize ear and certain parts of the brain. The ear consists of three components: outer ear, middle ear, and inner ear
The role of the outer ear – which includes external ear and ear canal – is to gather sound airwaves and transfer them to the middle ear.
The eardrum (also called the tympanic membrane) separates the outer ear from the middle ear. When sound waves hit the eardrum, it starts vibrating and transfers sound waves into mechanical movements of tiny bony structures inside the middle ear – called ossicles.
Movements of the ossicles stimulate a fluid-filled labyrinth of the inner ear called cochlea. Translation of sound waves energy into electrical and chemical signals takes place in the inner ear. Auditory signals get transferred by the auditory nerve to areas of the brain responsible for hearing.
Damage or malfunction of any of the ear components may result in hearing deficits or complete loss of hearing.
Causes of hearing problems
Hearing deficits can be congenital or acquired later in life. It is estimated that approximately 50% of congenital hearing loss is hereditary (Hereditary means that it is due to abnormal genes).
Mutations (mutations=abnormal changes) in gene GJB2 are the most common reason for non-syndromic severe hearing loss in babies born to parents who do not have a hearing problem.
Hearing problems that become apparent later on in life are usually due to:
- congenital infections (especially Cytomegalovirus)
- central nervous system infections (for example meningitis)
- genetic syndromes that become symptomatic later after birth
- chronic middle ear infections and effusions
- exposure to certain harmful medications
- exposure to a high level of noise
- head traumas
Simplifying; hearing problems can be due to conduction issues or due to the problems with signal processing in the inner ear, nerves, or areas of the brain.
Conduction issues may be caused by abnormal anatomy of the outer and middle ear or be due to infections and effusions in the middle ear.
Risk factors for hearing deficits
In 1973, the Joint Committee on Infant Hearing (JCIH) published the first set of risk factors for hearing deficits in children. (Link here)
These risk criteria have been updated several times, and the last available list is from the 2007 JCIH position statement. (Ref. 1).
Congenital and Acquired Hearing Loss Risk Factors (modified list):
- Caregiver concern regarding hearing, speech or language
- Family history of hearing loss
- Stay in NICU for more than 5 days
- Treatment with ECMO during the newborn period
- Treatment with Assisted ventilation
- Treatment with: gentamicin, tobramycin, or furosemide
- Hyperbilirubinemia (jaundice) that needed treatment with exchange transfusion
- Infections during pregnancy (CMV, Herpes, Rubella, Syphilis, Toxoplasmosis)
- Congenital anomalies of face and head
- Physical findings on the exam such as white forelock
- Syndromes associated with hearing loss (neurofibromatosis, osteopetrosis, Usher, Alport, Pendred, Jervell, Lange-Nielson)
- Neurodegenerative diseases: Hunter syndrome, Friedrich ataxia, and Charcot-Marie-Tooth syndrome
- Culture-positive postnatal infections: Herpes, Varicella, and bacterial and viral meningitis
- Head traumas – especially of the basal skull or temporal bone fracture
- Need for chemotherapy due to cancer
Newborn hearing screening tests
According to recommendations issued by various organizations, all newborns should undergo hearing screening tests in the hospital before discharge home. If a baby was born at home, a screening test should be done by the end of the first month of age.
Many reports indicate that when infants who have congenital hearing deficits without any other disabilities receive early intervention by the age of six months, they will have similar development of communication skills to hearing children.
Current recommendations are that we need to screen for hearing deficits by the age of 1 month, detect hearing deficit by the age of 3 months, and institute treatment by six months of age.
As of 2014, over 97% of babies in the US have been screened for hearing deficits each year at birth. If your baby was born in the US, and you are not aware of the hearing test results, you should confirm with your pediatrician that the test was indeed done.
Hospitals can use one of two available methods to screen newborns for hearing deficits: OEA or AABR.
OAE – utilizes the detection of otoacoustic emissions that are created in the inner ear in response to a stimulus. The absent or abnormal OEA may indicate an abnormality in the cochlea (inner ear), but it may also be due to problems in the middle ear (fluid effusion) or in the outer ear (wax, or anatomical abnormalities)
AABR stands for automated auditory brainstem responses. It is a newer technique that is recommended, especially for babies that needed to stay in the NICU or have other risks for hearing problems.
The AABR method is better for screening purposes because it allows the detection of responses from the auditory nerve and auditory portions of the brain as well.
Both screening methods are straightforward to administer. The baby can be asleep during the whole procedure. Ideally, the baby shouldn’t be fussy or hungry when the test is performed. The tester – usually a nurse – places a small probe in or near the baby’s ear to create the sound, and the computer will read the ear’s response to the generated stimuli (see the featured image above).
Some hospitals have apparatus that can perform a hearing test using both methods (OAE and AABR); others utilize only one of them. You should know that if your baby has one or more risk factors for hearing deficits listed above, the preferred technique to screen for hearing deficits is the AABR method.
What if my child failed the newborn hearing screening test?
A failed newborn hearing test means that your baby needs further diagnostic procedures that need to be done promptly.
A failed newborn hearing screening test does not say yet that your baby can not hear (It is called “screening”). Abnormal results may be due to baby’s fussiness, middle ear effusion, or obstruction in the outer ear canal.
At a minimum, if a baby failed the initial newborn hearing test, such a baby must have a repeat test within one month. If the test is still abnormal, the baby needs to be evaluated by ENT or audiology by three months of age. Each hospital, state, or country may have different guidelines on that, so you are always advised to check with your doctor.
My child passed the newborn hearing screening test; what does it mean?
If your child passed the newborn hearing screening test, it means that most likely, your child does not have a significant hearing problem.
The emphasis here is on “most likely.” Hearing screening test does not guarantee 100% accuracy. It is always possible that a small percentage of babies with already existing hearing deficits will not be detected.
I have explained earlier that some hereditary and acquired hearing deficits develop later in life. Parents have to be always vigilant and watch for any signs of a delay in language and communication skills.
If my child has been diagnosed with a hearing deficit; what can be done about it?
Whenever a baby is diagnosed with a permanent hearing deficit, referral to an appropriate audiology specialist should be done. The goal here is to obtain and fit a suitable amplification hearing device so the child can have a better chance of achieving good language outcomes.
For some children with hearing problems due to anatomical abnormality, surgery may be indicated.
Children with severe hearing deficits that did not benefit from amplification devices after at least six months of using them should be considered for cochlear implants.
It is advisable not to wait for too long with the decision to place a cochlear implant. Studies showed that children who receive their implants by twelve months of age have better language and communication outcomes than children who receive them between 13 and 24 months.
Summary:
A functioning hearing affects child’s development and cognition. All hearing deficits must be diagnosed as early as possible to facilitate early intervention. Newborn screening tests reveal only 50% of all hearing deficits in children. Any signs of delayed speech or cognition during a child’s life should prompt a reevaluation of hearing ability.
References:
- JCIH 2007 Position Statement
Disclaimer:
This article is only for general information purposes. It should not be viewed as any medical advice. There is a small chance that information here may be inaccurate. You should always discuss all health-related matters with your doctor before making any decisions that may affect your health or health of your family members.